0% found this document useful (0 votes)
63 views3 pagesApplication Form 1
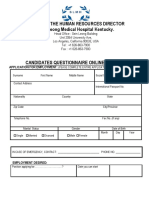
This document is an application for employment at South Coast Nursing Homes Ltd. It requests personal details such as name, address, phone number, date of birth, next of kin information. It also asks for education history, training history, employment history including current and previous employers, dates of employment, and positions held. Finally, it inquires about availability including notice period required, date available to start, and eligibility to work in the UK.
Uploaded by
Severino ValerioCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
63 views3 pagesApplication Form 1
This document is an application for employment at South Coast Nursing Homes Ltd. It requests personal details such as name, address, phone number, date of birth, next of kin information. It also asks for education history, training history, employment history including current and previous employers, dates of employment, and positions held. Finally, it inquires about availability including notice period required, date available to start, and eligibility to work in the UK.
Uploaded by
Severino ValerioCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
/ 3