0% found this document useful (0 votes)
853 views2 pagesUworld Biostatistics
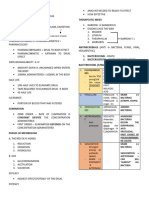
The document discusses key concepts in clinical trials and statistical analysis:
1. Randomization and blinding are used in clinical trials to minimize bias and confounding. Intention-to-treat analysis maintains the randomization.
2. Statistical distributions can be used to standardize data using z-scores.
3. Groups can be compared using t-tests, ANOVA, chi-square or Fisher's exact test depending on the type and size of the samples.
4. Statistical power depends on the alpha level, magnitude of difference between groups, and sample size. Larger samples and differences increase power while stricter criteria decrease power.
Uploaded by
Костянтин РоманівCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
853 views2 pagesUworld Biostatistics
The document discusses key concepts in clinical trials and statistical analysis:
1. Randomization and blinding are used in clinical trials to minimize bias and confounding. Intention-to-treat analysis maintains the randomization.
2. Statistical distributions can be used to standardize data using z-scores.
3. Groups can be compared using t-tests, ANOVA, chi-square or Fisher's exact test depending on the type and size of the samples.
4. Statistical power depends on the alpha level, magnitude of difference between groups, and sample size. Larger samples and differences increase power while stricter criteria decrease power.
Uploaded by
Костянтин РоманівCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
/ 2