0% found this document useful (0 votes)
72 views6 pagesPostpartum Hemorrhage Guide
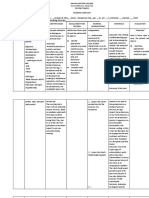
The document discusses postpartum hemorrhage and provides a nursing diagnosis of deficient fluid volume related to excessive blood loss after birth. Therapeutic management includes using pharmacological agents and clotting factor concentrates to improve hemostasis and decrease bleeding. Outcome evaluation focuses on maintaining stable vital signs and fluid balance.
The document also describes three types of lacerations that can occur during childbirth from first to third degree and provides the corresponding nursing diagnoses, therapeutic management, and outcome evaluations for each.
Uploaded by
Clare AlcoberCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
72 views6 pagesPostpartum Hemorrhage Guide
The document discusses postpartum hemorrhage and provides a nursing diagnosis of deficient fluid volume related to excessive blood loss after birth. Therapeutic management includes using pharmacological agents and clotting factor concentrates to improve hemostasis and decrease bleeding. Outcome evaluation focuses on maintaining stable vital signs and fluid balance.
The document also describes three types of lacerations that can occur during childbirth from first to third degree and provides the corresponding nursing diagnoses, therapeutic management, and outcome evaluations for each.
Uploaded by
Clare AlcoberCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
/ 6