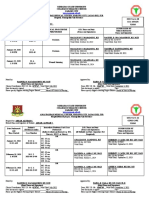
MEDICAL COLLEGES OF NORTHERN PHILIPPINES
Alimannao Hills, Peñablanca Cagayan
Telefax number: 078-3041010/ E-mail address: adminoffice@mcnp.edu.ph / Web site: www.mcnp.edu.ph
Accreditation Level: IQuAME CATEGORY A (t) MATURE TEACHING INSTITUTION/PACUCOA Accredited Level 2
SURGICAL SCRUB in _________________________________________________________________________
Hospital, Municipality/City/ Province
O.R. Form 1A
Prepared by: O.R. SCRUB FORM
Printed Name with Signature of student _________________________________________________________________ MAJOR
Date Performed Patients INITIALS (ONLY) SURGICAL PROCEDURE O.R. Nurse On Duty SUPERVISED BY
and PERFORMED (Name and Signature) Clinical Instructor
CASE NUMBER
Time Started Name and Signature
MEDICAL COLLEGES OF NORTHERN PHILIPPINES
Noted by: Approved by:
____NINA ANNE BERNADETTE P. PARACAD, RN, MSN____ LOUISE V. CABLING, RN, MAN, MST
Signature Over Printed Name of Clinical Coordinator Signature Over Printed Name of Dean
Date Signed: ______________________________ Date Signed: ________________________________
Degree: __________________________________ Degree: ____________________________________
a. PRC No.: _______________________ a. PRC No.:___________________________
Valid until:______________________ Valid Until:_________________________
b. PNA No.:________________________ b. PNA No.:___________________________
Valid until:______________________ Valid Until:_________________________
c. ADPCN No.:________________________
Valid Until:_________________________
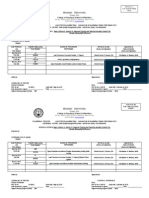
� Alimannao Hills, Peñablanca Cagayan
Telefax number: 078-3041010/ E-mail address: adminoffice@mcnp.edu.ph / Web site: www.mcnp.edu.ph
Accreditation Level: IQuAME CATEGORY A (t) MATURE TEACHING INSTITUTION/PACUCOA Accredited Level 2
SURGICAL SCRUB in _________________________________________________________________________
Hospital, Municipality/City/ Province
O.R. Form 1B
Prepared by: O.R. CIRCULATING FORM
Printed Name with Signature of student _________________________________________________________________ MINOR
Date Performed Patients INITIALS SURGICAL PROCEDURE O.R. Nurse On Duty SUPERVISED BY
and (ONLY) PERFORMED (Name and Signature) Clinical Instructor
Time Started CASE NUMBER Name and Signature
MEDICAL COLLEGES OF NORTHERN PHILIPPINES
Alimannao Hills, Peñablanca Cagayan
Noted by: Approved by:
____NINA ANNE BERNADETTE P. PARACAD, RN, MSN____ LOUISE V. CABLING, RN, MAN, MST
Signature Over Printed Name of Clinical Coordinator Signature Over Printed Name of Dean
Date Signed: ______________________________ Date Signed: ________________________________
Degree: __________________________________ Degree: ____________________________________
a. PRC No.: _______________________ a. PRC No.:___________________________
Valid until:______________________ Valid Until:_________________________
b. PNA No.:________________________ b. PNA No.:___________________________
Valid until:______________________ Valid Until:_________________________
c. ADPCN No.:________________________
Valid Until:_________________________
� Telefax number: 078-3041010/ E-mail address: adminoffice@mcnp.edu.ph / Web site: www.mcnp.edu.ph
Accreditation Level: IQuAME CATEGORY A (t) MATURE TEACHING INSTITUTION/PACUCOA Accredited Level 2
ACTUAL DELIVERY in ___________________________________________________________________________________
Hospital, Municipality/City/ Province
Prepared by: D.R FORM
Printed Name with Signature of student _________________________________________________________________ ACTUAL DELIVERY
FORM
Date Performed Patients INITIALS (ONLY) D.R. Nurse On Duty SUPERVISED BY
and CASE NUMBER PROCEDURE (Name and Signature) Clinical Instructor
Time Started (not applicable for birthing/lying- PERFORMED (IF Midwife on duty, Signature Name and Signature
in Clinics/Homes) not required)
MEDICAL COLLEGES OF NORTHERN PHILIPPINES
Alimannao Hills, Peñablanca Cagayan
Telefax number: 078-3041010/ E-mail address: adminoffice@mcnp.edu.ph / Web site: www.mcnp.edu.ph
Noted by: Approved by:
____NINA ANNE BERNADETTE P. PARACAD, RN, MSN____ LOUISE V. CABLING, RN, MAN, MST
Signature Over Printed Name of Clinical Coordinator Signature Over Printed Name of Dean
Date Signed: ______________________________ Date Signed: ________________________________
Degree: __________________________________ Degree: ____________________________________
a. PRC No.: _______________________ a. PRC No.:___________________________
Valid until:______________________ Valid Until:_________________________
b. PNA No.:________________________ b. PNA No.:___________________________
Valid until:______________________ Valid Until:_________________________
c. ADPCN No.:________________________
Valid Until:_________________________
� Accreditation Level: IQuAME CATEGORY A (t) MATURE TEACHING INSTITUTION/PACUCOA Accredited Level 2
ACTUAL DELIVERY in ___________________________________________________________________________________
Hospital, Municipality/City/ Province
Prepared by: D.R FORM
Printed Name with Signature of student _________________________________________________________________ ASSISSTED DELIVERY
FORM
Date Performed Patients INITIALS (ONLY) D.R. Nurse On Duty SUPERVISED BY
and CASE NUMBER PROCEDURE (Name and Signature) Clinical Instructor
Time Started (no applicable for birthing/lying-in PERFORMED (IF Midwife on duty, Signature Name and Signature
Clinics/Homes) not required)
MEDICAL COLLEGES OF NORTHERN PHILIPPINES
Alimannao Hills, Peñablanca Cagayan
Telefax number: 078-3041010/ E-mail address: adminoffice@mcnp.edu.ph / Web site: www.mcnp.edu.ph
Accreditation Level: IQuAME CATEGORY A (t) MATURE TEACHING INSTITUTION/PACUCOA Accredited Level 2
Noted by: Approved by:
____NINA ANNE BERNADETTE P. PARACAD, RN, MSN____ LOUISE V. CABLING, RN, MAN, MST
Signature Over Printed Name of Clinical Coordinator Signature Over Printed Name of Dean
Date Signed: ______________________________ Date Signed: ________________________________
Degree: __________________________________ Degree: ____________________________________
a. PRC No.: _______________________ a. PRC No.:___________________________
Valid until:______________________ Valid Until:_________________________
b. PNA No.:________________________ b. PNA No.:___________________________
Valid until:______________________ Valid Until:_________________________
c. ADPCN No.:________________________
Valid Until:_________________________
� ACTUAL DELIVERY in ___________________________________________________________________________________
Hospital, Municipality/City/ Province
Prepared by: ICBN FORM
Printed Name with Signature of student _________________________________________________________________ IMMEDIATE CARE OF THE
NEWBORN FORM
Date Performed Patients INITIALS (ONLY) IMMEDIATE NEW BORN CORD CARE D.R. Nurse On Duty SUPERVISED BY
and CASE NUMBER PERFORMED (Name and Signature) Clinical Instructor
Time Started (not applicable for birthing/lying-in Indicate where it is performed e.g. D.R., (IF Midwife on duty, Signature Name and Signature
Clinics/Homes) Nursery, NICU, or HOME not required)
Noted by: Approved by:
____NINA ANNE BERNADETTE P. PARACAD, RN, MSN____ LOUISE V. CABLING, RN, MAN, MST
Signature Over Printed Name of Clinical Coordinator Signature Over Printed Name of Dean
Date Signed: ______________________________ Date Signed: ________________________________
Degree: __________________________________ Degree: ____________________________________
a. PRC No.: _______________________ a. PRC No.:___________________________
Valid until:______________________ Valid Until:_________________________
b. PNA No.:________________________ b. PNA No.:___________________________
Valid until:______________________ Valid Until:_________________________
c. ADPCN No.:________________________
Valid Until:_________________________