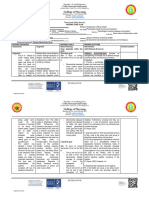
Subjective data:
- “ginregla ko duwa ka semana kag damo ang ga gwa sa akon nga dugo, dason gauntat
sa after 5 days mabalik naman nga da patak-patak”
Objective data:
- decreased hemoglobin and hematocrit count
- profuse menstruation
Nursing Diagnosis
Deficient fluid volume related to blood loss as evidenced by vaginal bleeding for 2weeks,
decreased hemoglobin and hematocrit result
Goal:
After 2 days of nursing intervention, client will be able to:
a. Experience adequate fluid volume and electrolyte balance.
Nursing Interventions
DEPENDENT
a. Assess for laboratory studies, such as complete blood count (CBC), electrolyte levels,
and renal function tests, as indicated.
- Regular monitoring of laboratory values helps assess the severity of fluid
volume deficit, guide appropriate fluid replacement therapies, and monitor the
client’s response to treatment. The hematocrit level is greater than normal
because there is a decreased plasma volume.
b. Administer appropriate medication as ordered.
- Administer antipyretics, and antiemetic to reduce fluid loss, if the patient
experiences ongoing vomiting.
c. Start parenteral fluid therapy per order and perform a fluid challenge if ordered.
- Intravenous fluids ensure more consistent hydration than oral fluid intake.
Physicians perform fluid challenges to see if the patient has a preload reserve
that can be used to improve cardiac function and fluid status.
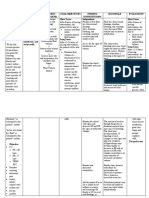
�INDEPENDENT
a. Monitor active fluid loss from wound drainage, tubes, diarrhea, bleeding, and vomiting
- Maintain accurate input and output.
b. Monitor for presence of nausea, vomiting, and fever.
- Nausea, vomiting, and fever can lead to fluid losses and contribute to fluid volume
deficit. Gastroenteritis is the most common cause of dehydration. If both vomiting and
diarrhea are present, dehydration may rapidly progress.
c. Monitor serum electrolytes and urine osmolality and report abnormal values.
- Elevated hemoglobin and elevated blood urea nitrogen (BUN) suggest fluid
deficit. Urine-specific gravity is likewise increased.
d. Palpate bladder. Investigate reports of discomfort, fullness, inability to void.
- Perception of bladder fullness, distention of bladder above symphysis pubis
indicates urinary retention.
e. Encourage patient to drink prescribed fluid amounts
- Oral fluid replacement is indicated for mild fluid deficit.
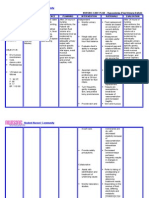
COLLABORATIVE
a. Catheterize when indicated/per protocol if patient is unable to void or is uncomfortable.
- Edema or interference with nerve supply may cause bladder atony/urinary
retention requiring decompression of the bladder. Note: Indwelling urethral or
suprapubic catheter may be inserted intraoperatively if complications are
anticipated.
b. Collaborate with the dietitian to develop a balanced diet plan that meets the client’s
nutritional needs while considering fluid restrictions, if applicable.
- Adequate nutrition supports overall health and helps optimize fluid balance.
Dietitians can develop personalized meal plans that take into account the client’s
fluid restrictions or preferences. They can help identify foods and beverages that
are hydrating and provide necessary electrolytes.
c. Assist the physician with insertion of a central venous line and arterial line as indicated.
- This allows more effective fluid administration and monitoring.
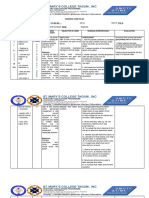
HEALTH TEACHING
a. Educate the client and family members about the importance of maintaining hydration
and recognizing signs of fluid volume deficit.
� - Client and family education promotes understanding of the condition, encourages
adherence to fluid replacement strategies, and enables early detection of fluid
volume deficit. By increasing awareness, clients can recognize the early warning
signs such as increased thirst, dry mouth, dark urine, dizziness, fatigue, and
confusion. Timely recognition allows for prompt intervention and prevents the
progression of these conditions to more severe stages.
b. Emphasize the relevance of maintaining proper nutrition and hydration.
- Increasing the client’s knowledge level will assist in preventing and managing the
problem. Hydration and nutrition are the interventions with the greatest impact on
the course of acute diarrhea. Traditional clear fluids are not appropriate for oral
rehydration therapy. Many contain excessive concentrations of carbohydrates and
low concentrations of sodium. This could further worsen the degree of
dehydration (Huang & Corden, 2018).
c. Inform caregivers and family members to provide support to the client.
- Findings from a study suggest that family presence during emergencies and
procedures is beneficial to the client. Nurses should identify with the client which
family member should be present should a life-threatening event occur. Nurses
have a key role in supporting family members who are present during life-
threatening events. Nurses can assist families in understanding life-threatening
events as they unfold, providing support to families during crises.