0% found this document useful (0 votes)
476 views4 pagesSBFP PTR Template
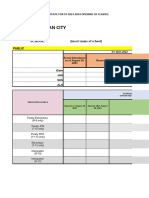
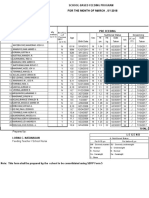
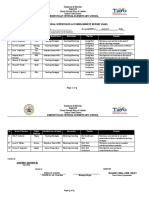
This document is a program terminal report form for the School-Based Feeding Program (SBFP) in COTABATO/CARMEN CENTRAL covering SY 2023-2024. It provides data on the number of beneficiaries in the program pre-feeding and post-feeding, including beneficiaries by grade level and nutritional status. It also lists the types and quantities of food commodities distributed. The form requests information on donations/resources generated, significant events, lessons learned, proposed plans and recommendations.
Uploaded by
Liza BacudoCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as XLSX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
476 views4 pagesSBFP PTR Template
This document is a program terminal report form for the School-Based Feeding Program (SBFP) in COTABATO/CARMEN CENTRAL covering SY 2023-2024. It provides data on the number of beneficiaries in the program pre-feeding and post-feeding, including beneficiaries by grade level and nutritional status. It also lists the types and quantities of food commodities distributed. The form requests information on donations/resources generated, significant events, lessons learned, proposed plans and recommendations.
Uploaded by
Liza BacudoCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as XLSX, PDF, TXT or read online on Scribd
/ 4