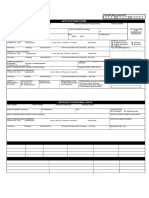
CITY GOVERNMENT OF PASIG
Person with Disability Affairs Office PDAO
DEPARTMENT OF HEALTH
Philippine Registry for Person With Disability Version 3.0
NEW: _______ RENEWAL: _______ LOST: _______ REPLACEMENT: ________ TRANSFER: _________
1. PERSONS WITH DISABILITY NUMBER (RR-PPMM-BBB-NNNNNNN)* 2. DATE APPLIED:*
Place 1x1
3. PERSONAL INFORMATION*
Photo Here
LAST NAME:* FIRST NAME:* MIDDLE NAME:* SUFFIX:
4. DATE OF BIRTH * AGE: * 5. RELIGION: 6. ETHNIC GROUP
7. SEX: * 8. CIVIL STATUS: * 9. BLOOD TYPE:
Male Single Married Widower A+ AB+ B+ O+
Female Widow/er Cohabitation (live-in) A- AB- B- O-
10. TYPE OF DISABILITY: * 11. CAUSE OF DISABILITY: *
Acquired
Deaf or Hard of Hearing Physical Disability Cancer
Intellectual disability Psychosocial Disability Chronic Illness
Learning Disability Speech and Language Impairment Congenital/Inborn
Mental Disability Visual Disability Injury
Orthopedic Disability Rare Disease
Autism
12. RESIDENCE ADDRESS *
House No. And Street:* Barangay:* Municipality: * Province: * Region: *
13: CONTACT DETAILS
Landline Number: Mobile Number: Email Address:
14. EDUCATIONAL ATTAINMENT: * 15. STATUS OF EMPLOYMENT: * 16. OCCUPATION: *
Employed Managers
None Unemployed Professionals
Elementary Education Self-employed Technician and Associate Professionals
High School Education 15a. CATEGORY OF EMPLOYEMENT: * Clerical Support Workers
College Government Service and Sales Workers
Postgraduate Program Private Skilled Agricultural, Forestry & Fishery Workers
Non-Formal Education Plant and Machine Operators & Assemblers
15b. TYPES OF EMPLOYMENT:*
Vocational Elementary Occupations
Permanent/Regular
Armed Forces occupations
Seasonal
Others, specify:
Casual
______________________________
Emergency
17. ORGANIZATION INFORMATION:
Organization Affiliated: Contact Person: Office Address: Tel. Nos.:
18. ID REFERENCE NO.:
SSS NO.: GSIS NO.: Pag-IBIG NO.: PHILhEALTH NO.:
19. FAMILY BACKGROUND LAST NAME FIRST NAME MIDDLE NAME
FATHER’S NAME:
MOTHER’S NAME:
GUARDIAN’S NAME:
20. ACCOMPLISHED BY: *
20A. NAME OF REPORTING UNIT:
21. REGISTRATION NUMBER:
APPLICATION REQUIREMENTS
FOR NEW APPLICANT
PWD Application Form 2pcs 1x1 ID picture Xerox copy of
Recent Medical Certificate of Disability with Doctor’s 1 whole body picture holding valid ID issued by
Signature, PTR & License Number a recent calendar (proof of the govt. showing
Voter’s ID/Registration life) the date of birth
Brgy. Certificate (if not a registered voter of Pasig City) Copy of Birth Certificate of the applicant.
FOR ID RENEWAL
PWD Application Form 2pcs 1x1 ID picture Xerox copy of valid ID
Old or New Medical Certificate of Disability with Doctor’s 1 whole body picture issued by the govt.
Signature, PTR & License Number holding a recent calendar showing the date
Voter’s ID/Registration (proof of life) of birth of the
Copy of Birth Certificate applicant.
FOR LOST ID: Please submit application form, copy of medical certificate, proof of life (picture with recent calendar) and affidavit of loss.
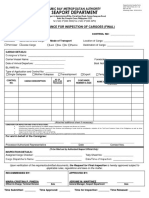
�WALK IN _____ BARANGAY _____ ONLINE _____ ENDORSED _____ _________________
NEW: _____ RENEWAL: _____ LOST: _____ REPLACEMENT: _____ TRANSFER: _____ 1x1 picture
NAME: _________________________________________ AGE: _____ CTRL NO. __________
LAST NAME NAME MIDDLE NAME
PWD NUMBER: __________________________________ BARANGAY: ___________________________
TYPE OF DISABILTY: _________________________________DIAGNOSIS: ______________________________
ADDRESS: ________________________________________________________________________________
Contact Number: ________________________ DATE OF BIRTH: _______________GENDER: ________________
Month/Date/Year Male/Female
Email Address: ______________________________ Mother's Maiden Name: _____________________________
In case of emergency please notify:
Name: ___________________________ Relationship: _________________ Contact Number: ________________
I __________________________________ resident of Barangay _______________, Pasig City agreed to consent by
submitting this reply form; consent to the collection, generation, use, processing, storage and retention of my personal
data by PDAO for the purpose(s) described in this document. Please ensure that you have completely read and
understood the terms before signing. Any change will not be applied and will not alter how PDAO handles previously
collected personal data without obtaining your consent, unless required by law.
Date: __________________________ Signature: _____________________________
The Republic Act No. 10173, or the Data Privacy Act of 2012 (DPA), with the National Privacy Commission (NPC) overseeing its proper implementation.
REMARKS:
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
_____________________________________________________________________________