GIDA Information System Toolkit, 2018 version
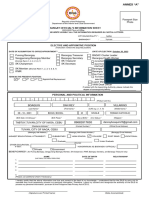
IV. GIDA Profiling Tool
A. General Information
REFERENCE YEAR
___ ___ ___ ___
(Specify the year for the basis of data)
G001 BARANGAY NAME
G002 MUNICIPALITY / CITY NAME
G003 PROVINCE NAME
G004 REGION NAME
G005 BARANGAY DESCRIPTION UPLAND ISLAND LANDLOCKED LOWLAND OTHERS, SPECIFY:
TOTAL NUMBER OF PUROK/SITIO/ZONE IN THE
G006 BARANGAY (Whichever is being used to identify
the next lower classification to barangay)
G007 TOTAL BARANGAY IRA AND OTHER INCOME P ___________________
G008a LAND AREA in hectares ___________________ hectares
G008b LAND AREA in sq. km. ___________________ square kilometers
ARE THERE ANY COMMUNITIES AFFECTED BY
G009a YES NO
CONFLICT IN THE BARANGAY? (if no, skip to G010)
NO. OF PUROK/SITIO/ZONE WITH ARMED
G009b
CONFLICT
ESTIMATED % OF POPULATION THAT ARE
G009c ______ %
AFFECTED BY CONFLICT
ARE THERE INTERNALLY DISPLACED PERSONS
G010a YES NO
(IDP) IN THE BARANGAY? (if no, skip to G011)
G010b NO. OF PUROK/SITIO/ZONE WITH IDP
G010c ESTIMATED % of POPULATION THAT ARE IDPs ______ %
IS THERE AN ICC/IP IN THE BARANGAY? (if no,
G011a YES NO
skip to G013)
G011b NO. OF PUROK/SITIO/ZONE WITH ICC/IP
G012 MAJOR ETHNOLINGUISTIC GROUP/S (specify all)
G013 IS THERE A BARANGAY HEALTH BOARD? YES NO (If no, skip to G016)
40
� GIDA Information System Toolkit, 2018 version
IS THE BARANGAY HEALTH BOARD MEETING Monthly Quarterly Semi Annual Annual No regular meeting
G014
REGULARLY?
Others, Specify _______
ARE ICCs/IPs REPRESENTED IN THE BARANGAY
G015 YES NO
HEALTH BOARD?
UTILIZATION OF ICLINICSYS OR OTHER
G016 YES NO
ELECTRONIC MEDICAL RECORD (BHS level)
B. Barangay Vital Statistics / Health Data
ALL IP
V001 TOTAL ACTUAL POPULATION
V002 TOTAL PROJECTED POPULATION
V003 TOTAL NUMBER OF HOUSEHOLDS
POPULATION BY AGE-GROUP MALE FEMALE MALE FEMALE
V004A UNDER 1 YR.
V004B 1 – 4 YRS.
V004C 5 – 9 YRS.
V004D 10 – 14 YRS.
V004E 15 - 19 YRS.
V004F 15 – 49 YRS.
V004G 50 – 59 YRS.
V004H 60 YRS. AND ABOVE
V005 TOTAL NUMBER OF PREGNANT WOMEN WITH 4 OR MORE PRENATAL VISITS
V006 TOTAL NUMBER OF LIVEBIRTHS
V007 TOTAL NUMBER OF DELIVERIES (including facility and non-facility deliveries)
V008 TOTAL NUMBER OF FACILITY-BASED DELIVERIES
V009 TOTAL NUMBER OF DELIVERIES ATTENDED BY SKILLED BIRTH ATTENDANT
TOTAL NUMBER OF DELIVERIES (BOTH FACILITY AND NON-FACILITY) WITH LOW BIRTH
V010
WEIGHT
TOTAL NUMBER OF <15 YEARS OLD WHO HAD A LIVEBIRTH OR PREGNANT WITH FIRST
V011
CHILD
41
� GIDA Information System Toolkit, 2018 version
TOTAL NUMBER OF 15-19 YEARS OLD WHO HAD A LIVEBIRTH OR PREGNANT WITH FIRST
V012
CHILD
V013 TOTAL NUMBER OF FETAL DEATHS (death in the womb after 22 weeks of pregnancy)
V014 TOTAL NUMBER OF NEONATAL DEATHS (death during first 28 days of life)
V015 TOTAL NUMBER OF INFANT DEATHS (death before first year of age)
V016 TOTAL NUMBER OF UNDER 5 DEATHS
TOTAL NUMBER OF MATERNAL DEATHS (within 42 days after delivery/termination of
V017
pregnancy)
V018 TOTAL NUMBER OF DEATHS (BASED ON PLACE OF RESIDENCE)
V019 TOTAL NUMBER OF FULLY IMMUNIZED CHILDREN UNDER AGE 1 (as defined in FHSIS)
V020 TOTAL NUMBER OF FAMILY PLANNING- CURRENT USERS
V021 TOTAL NUMBER OF NHTS HOUSEHOLDS
V022 TOTAL NUMBER OF HOUSEHOLDS REGISTERED IN 4PS/CCT/MCCT
TOTAL NUMBER OF 4PS/CCT/MCCT HOUSEHOLDS ENROLLED IN PHILHEALTH
V023
(WITH/WITHOUT PHILHEALTH CARD)
C. Barangay Health Facility, Access to Referral Hospitals, Human Resources for Health, Available
Medicines
R000 NAME OF NEAREST RHU/MAIN HEALTH CENTER _____________________________________
Yes
No, specify name of nearest BHS serving the
R001 PRESENCE OF BARANGAY HEALTH STATION (If No, skip to R003)
Population _____________________________
_______________________________________
For repair and renovation
For upgrading
R002 PRESENT PHYSICAL STATUS OF BARANGAY HEALTH STATION BHS attached to another structure (e.g. Bgy.
Hall)
Others, please specify
___________________
RHU
Satellite Clinic
WHAT IS THE NEAREST REFERRAL FACILITY TO THE BARANGAY HEALTH STATION? Private Hospital
R003
(Nearest BHS If NO BHS in Barangay) Government Hospital
Others, please specify
___________________
HOW MANY HOURS (USUAL MODE OF TRAVEL) IS THE BARANGAY HEALTH STATION TO
R004 THE NEAREST REFERRAL FACILITY (RHU, SATELLITE CLINIC, PRIVATE/GOVERNMENT
HOSPITAL)? (Use nearest BHS as basis If NO BHS in Barangay) Hours Minutes
R005 PRESENCE OF A BIRTHING FACILITY (e.g. Lying-in, BEMONC) PUBLIC, with dedicated RM/RN 24/7
PUBLIC, with on call staff 24/7
42
� GIDA Information System Toolkit, 2018 version
PUBLIC, But no human resource
PRIVATE, with dedicated RM/RN 24/7
PRIVATE, with on call staff 24/7
NO BIRTHING FACILITY
Others, please specify _________________
With dedicated DOH RN at least 5
days/week
With visiting DOH RN at least once a week
With visiting DOH RN at least 2x/month
With visiting DOH RN at least 1/month
R006 NURSE AVAILABLE IN THE BARANGAY (WITH OR WITHOUT BHS) With dedicated LGU RN at least 5 days/week
With visiting LGU RN at least once a week
With visiting LGU RN at least 2x/month
With visiting LGU RN at least 1/month
Not available at all
Others, please specify _________________
With dedicated DOH RM at least 5
days/week
With visiting DOH RM at least once a week
With visiting DOH RM at least 2x/month
With visiting DOH RM at least 1/month
With dedicated LGU RM at least 5
R007 MIDWIFE AVAILABLE IN THE BARANGAY (WITH OR WITHOUT BHS)
days/week
With visiting LGU RM at least once a week
With visiting LGU RM at least 2x/month
With visiting LGU RM at least 1/month
Not available at all
Others, please specify _________________
R008 TOTAL NUMBER OF BARANGAY HEALTH WORKERS IN THE BARANGAY
HOW MANY PUROK/SITIO/ZONE ARE >60 MINUTES (BY WALKING) AWAY FROM BHS?
R009 (Denominator is the answer on G006 “Number of Purok/Sitio”; if NO BHS, use the
nearest BHS as basis)
HOW MANY PUROK/SITIO/ZONE ARE >60 MINUTES (BY ANY MODE OF TRANSPORT)
R010 AWAY FROM BHS? (Denominator is the answer on G006 “Number of Purok/Sitio”; if NO
BHS, use the nearest BHS as basis)
HOW MANY PUROK/SITIO/ZONE ARE >60 MINUTES (BY WALKING) AWAY FROM RHU?
R011
(Denominator is the answer on G006 “Number of Purok/Sitio”)
HOW MANY PUROK/SITIO/ZONE ARE >60 MINUTES (BY ANY MODE OF TRANSPORT)
R012
AWAY FROM RHU? (Denominator is the answer on G006 “Number of Purok/Sitio”)
HOW MANY PUROK/SITIO/ZONE ENCOUNTER SEASONAL ACCESSSIBILITY ISSUES (FROM
BHS) FOR AVERAGE 3 MONTHS OR MORE (IN A YEAR) (like raining, high/low tide,
R013
monsoon, flood, landslide, etc)? (Denominator is the answer on G006 “Number of
Purok/Sitio”)
HOW MANY PUROK/SITIO/ZONE ENCOUNTER SEASONAL ACCESSSIBILITY ISSUES (FROM
R014 RHU) FOR AVERAGE 3 MONTHS OR MORE (IN A YEAR) (like raining, high/low tide,
monsoon etc)? (Denominator is the answer on G006 “Number of Purok/Sitio”)
Always available (100% of the time)
AVAILABILITY OF ANTI-TB MEDICINES AT THE BARANGAY LEVEL (choose the statement
R015 Available most of the time (>50%)
that best describes the availability for the reference year)
Drug available sometimes (25-50%)
43
� GIDA Information System Toolkit, 2018 version
Drug rarely available (<50%)
Not available
Not available, not needed in the Barangay
Always available (100% of the time)
Available most of the time (>50%)
AVAILABILITY OF ANTI-HYPERTENSIVE MEDICINES AT THE BARANGAY LEVEL (choose the Drug available sometimes (25-50%)
R016
statement that best describes the availability for the reference year) Drug rarely available (<50%)
Not available
Not available, not needed in the Barangay
Always available (100% of the time)
Available most of the time (>50%)
AVAILABILITY OF ANTI-DIABETIC MEDICINES AT THE BARANGAY LEVEL (choose the Drug available sometimes (25-50%)
R017
statement that best describes the availability for the reference year) Drug rarely available (<50%)
Not available
Not available, not needed in the Barangay
D. Peace and Order Situation
Weekly
IF THERE ARE MILITARY OPERATIONS/INSURGENT ACTIVITIES IN THE BARANGAY, HOW OFTEN Monthly
P001
DID IT OCCUR? (Choose the frequency that best describes the situation in the barangay) Occasionally
None
P002 CURRENTLY, ARE THERE MILITARY DETACHMENTS IN THE AREA? Yes No
E. Health Status
TOP TEN LEADING CAUSES OF MORTALITY TOP TEN LEADING CAUSES OF MORBIDITY
CAUSE NUMBER OF CAUSE NUMBER OF CASES
CASES
1. 1.
2. 2.
3. 3.
4. 4.
5. 5.
6. 6.
7. 7.
8. 8.
9. 9.
10. 10.
44
� GIDA Information System Toolkit, 2018 version
F. Environmental Sanitation and Basic Services (All Population and IP)
ALL IP
TOTAL NUMBER OF HOUSEHOLDS WITH ACCESS TO IMPROVED
E001
WATER SUPPLY
E002 TOTAL NUMBER OF HOUSEHOLDS WITH SANITARY TOILET
E003 TOTAL NUMBER OF HOUSEHOLDS WITH ELECTRICITY (ESTIMATE)
24 HOURS/DAY
E004 ELECTRICITY PROVISION ≥12 HOURS/DAY
<12 HOURS/DAY
No electricity
5, VERY STRONG
4, STRONG
IN A SCALE OF 0 TO 5, RATE THE PRESENCE/STRENGTH OF THE 3, STRONG SOMETIMES
E005
INTERNET CONNECTION IN THE BARANGAY? 2, WEAK
1, VERY WEAK
0, NONE
5, VERY STRONG
4, STRONG
IN A SCALE OF 0 TO 5, RATE THE PRESENCE/STRENGTH OF THE
3, STRONG SOMETIMES
E006 MOBILE PHONE SIGNAL IN THE BARANGAY? (regardless of
2, WEAK
network provider)
1, VERY WEAK
0, NONE
G. Environmental Hazards
Proximity To Environmental Hazards
H001 IS THIS BARANGAY NEAR TO A KNOWN FAULT LINE? YES NO DON’T KNOW
H002 IS THIS BARANGAY A TYPHOON-PRONE AREA? YES NO
H003 IS THIS BARANGAY A FLOOD-PRONE AREA? YES NO
H004 IS THIS BARANGAY A LANDSLIDE-PRONE AREA? YES NO
H005 IS THIS BARANGAY A TSUNAMI-PRONE AREA? YES NO
H006 IS THIS BARANGAY NEAR AN ACTIVE VOLCANO? YES NO
H007 HAS BARANGAY EVER EXPERIENCED STORM SURGE? YES NO
45
� GIDA Information System Toolkit, 2018 version
H. Basic Facilities
Mission upon request
Mission once a year
Missions once every 6 months
Missions once every 3 months
I001 CONDUCT OF MEDICAL/DENTAL/SURGICAL MISSION (Choose only one)
Missions monthly
No missions
Others. Please specify:
O
______________________________
O
tVehicles (3 or 4 wheels)
thMotorboats/Sea Ambulance
h
eMotorbikes
erHuman or animal carrier
I004 AVAILABILITY OF REFERRAL TRANSPORT (Specify all that applies) Helicopter/Air Ambulance
rsNone. Only by walking
s.Others. Please specify: ________
.
_____________________________
P
P
l
Accomplished by: Attested by: Attested by (if Attested by: le Validated by:
applicable):
ea
Rural Health Midwife Barangay Chairman IP Tribal Leader/IPMR Municipal Health Officer s
a DMO
se
Date: ____________ Date: ____________ Date: ____________ Date: ____________ Date: ____________
e
Note: Please affix signature over printed name.
46