0% found this document useful (0 votes)
16 views1 pageE Request
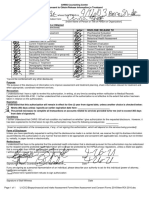
This document is an authorization form for the use and disclosure of protected health information by a patient. It includes sections for patient details, the healthcare provider releasing records, and the specific information to be disclosed. The form outlines the patient's rights regarding the authorization, including the right to revoke it and to inspect their health information.
Uploaded by
koushalya vCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
16 views1 pageE Request
This document is an authorization form for the use and disclosure of protected health information by a patient. It includes sections for patient details, the healthcare provider releasing records, and the specific information to be disclosed. The form outlines the patient's rights regarding the authorization, including the right to revoke it and to inspect their health information.
Uploaded by
koushalya vCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
/ 1