0% found this document useful (0 votes)
55 views4 pagesQuery Letter DownloadCFNetworkDownload RHzFw9
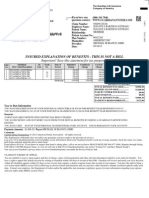
This document is a cashless authorization letter for a medical claim for the patient Iramganti Andalu, valid until 11/Aug/2025, with a total approved amount of Rs. 722475. The authorization covers a medical treatment for hypotension with an expected length of stay of 8 days in ICU. It outlines the terms and conditions for claim processing, including required documentation and exclusions for non-payable conditions.
Uploaded by
ankitvyas9368Copyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
55 views4 pagesQuery Letter DownloadCFNetworkDownload RHzFw9
This document is a cashless authorization letter for a medical claim for the patient Iramganti Andalu, valid until 11/Aug/2025, with a total approved amount of Rs. 722475. The authorization covers a medical treatment for hypotension with an expected length of stay of 8 days in ICU. It outlines the terms and conditions for claim processing, including required documentation and exclusions for non-payable conditions.
Uploaded by
ankitvyas9368Copyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
/ 4