0% found this document useful (0 votes)
115 views41 pagesConcept Map Format For CLA
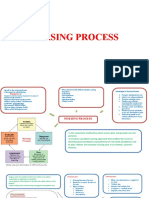
This document provides a sample concept map format for documenting a patient's plan of care using the nursing process. It includes sections for the patient's background information, three priority nursing diagnoses written in the NANDA format, relevant assessment findings, and goals and interventions. The concept map format allows nurses to visually map out the relationships between a patient's problems, diagnoses, and plan of care to guide clinical decision-making and nursing care.
Uploaded by
Adellaine Lois GreyCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PPT, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
115 views41 pagesConcept Map Format For CLA
This document provides a sample concept map format for documenting a patient's plan of care using the nursing process. It includes sections for the patient's background information, three priority nursing diagnoses written in the NANDA format, relevant assessment findings, and goals and interventions. The concept map format allows nurses to visually map out the relationships between a patient's problems, diagnoses, and plan of care to guide clinical decision-making and nursing care.
Uploaded by
Adellaine Lois GreyCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PPT, PDF, TXT or read online on Scribd
/ 41