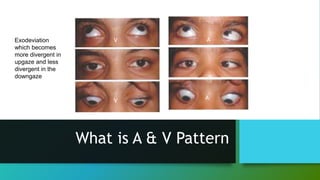
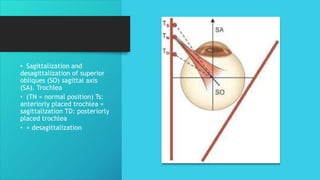
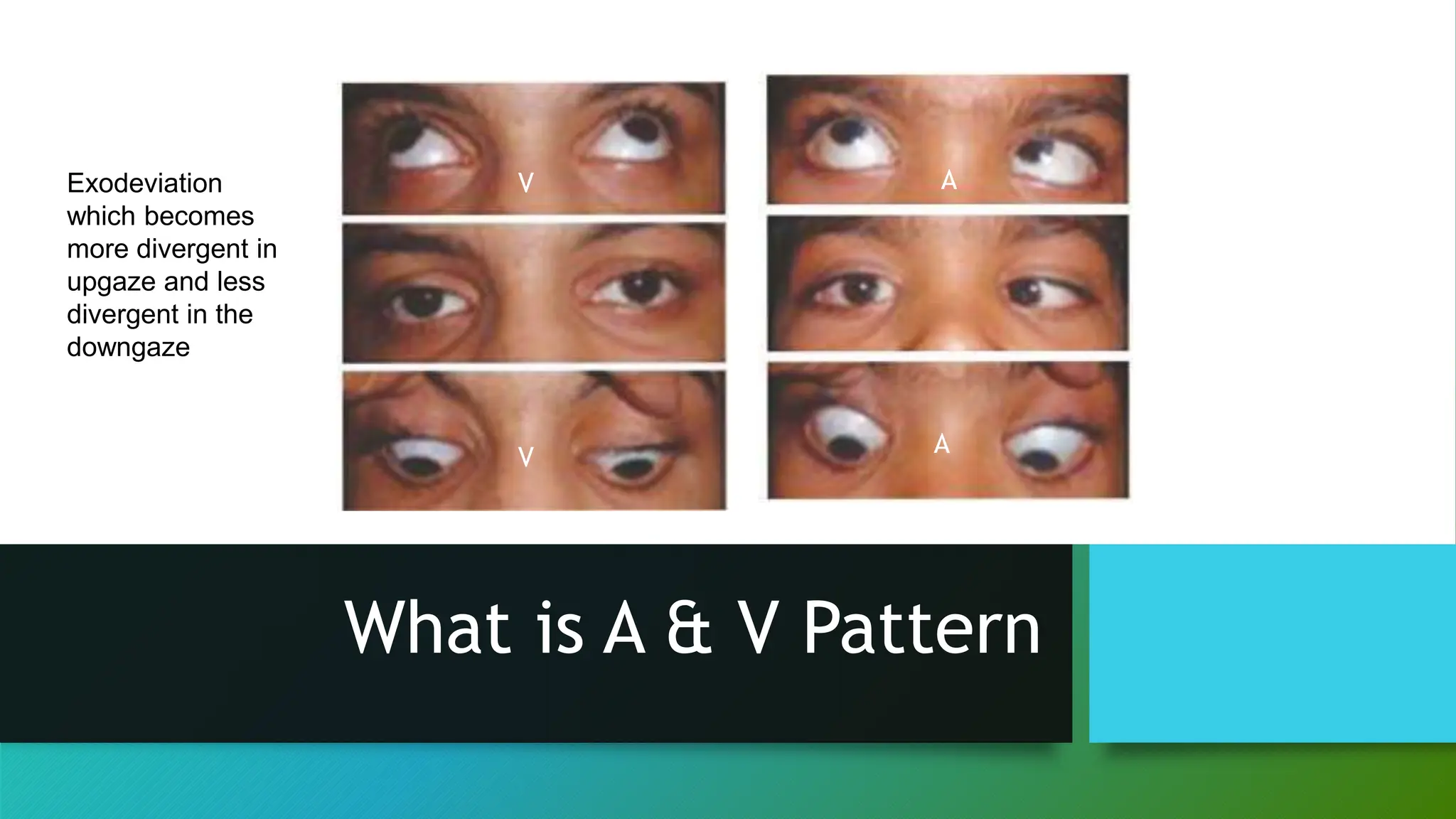
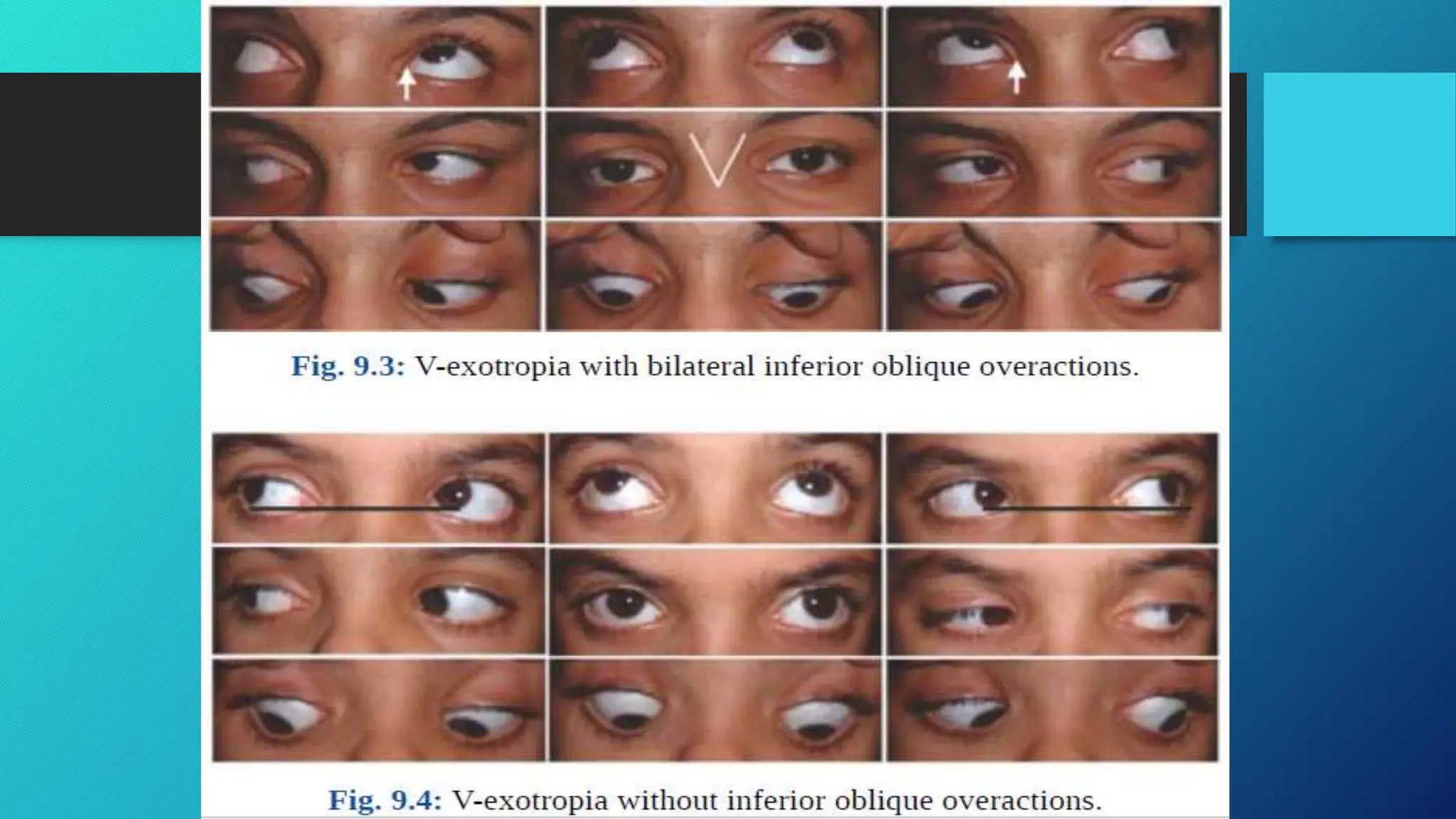
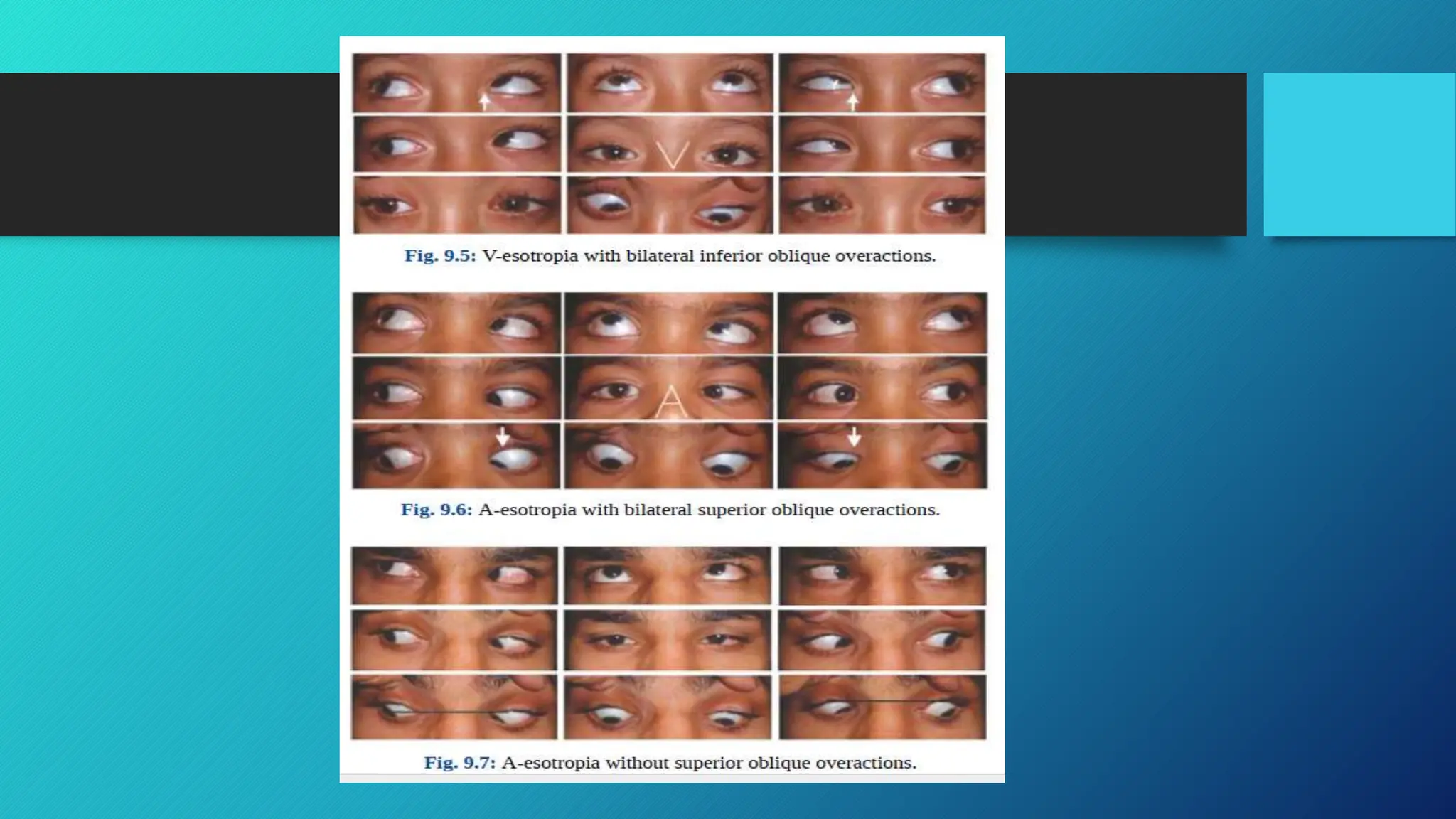
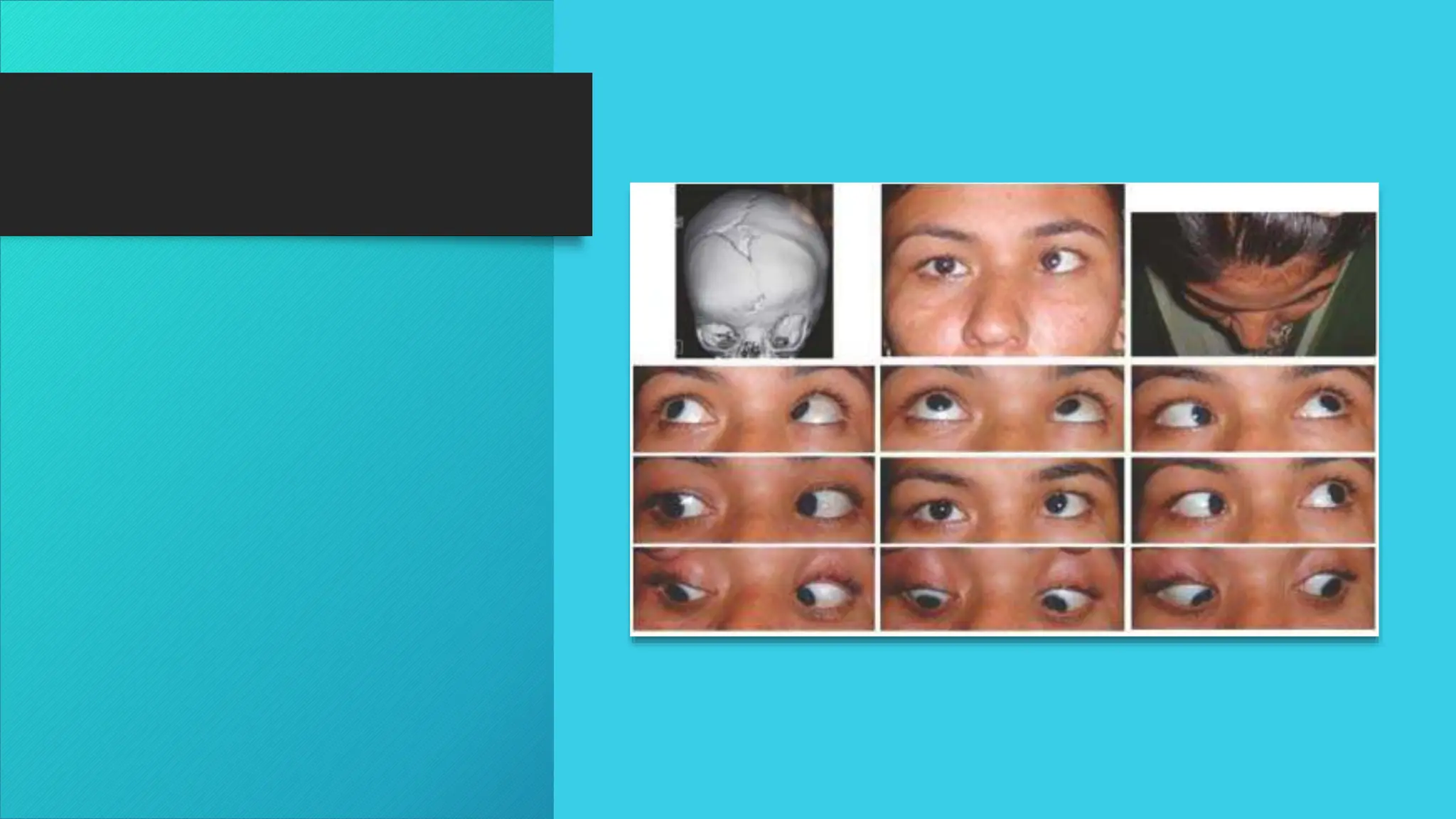
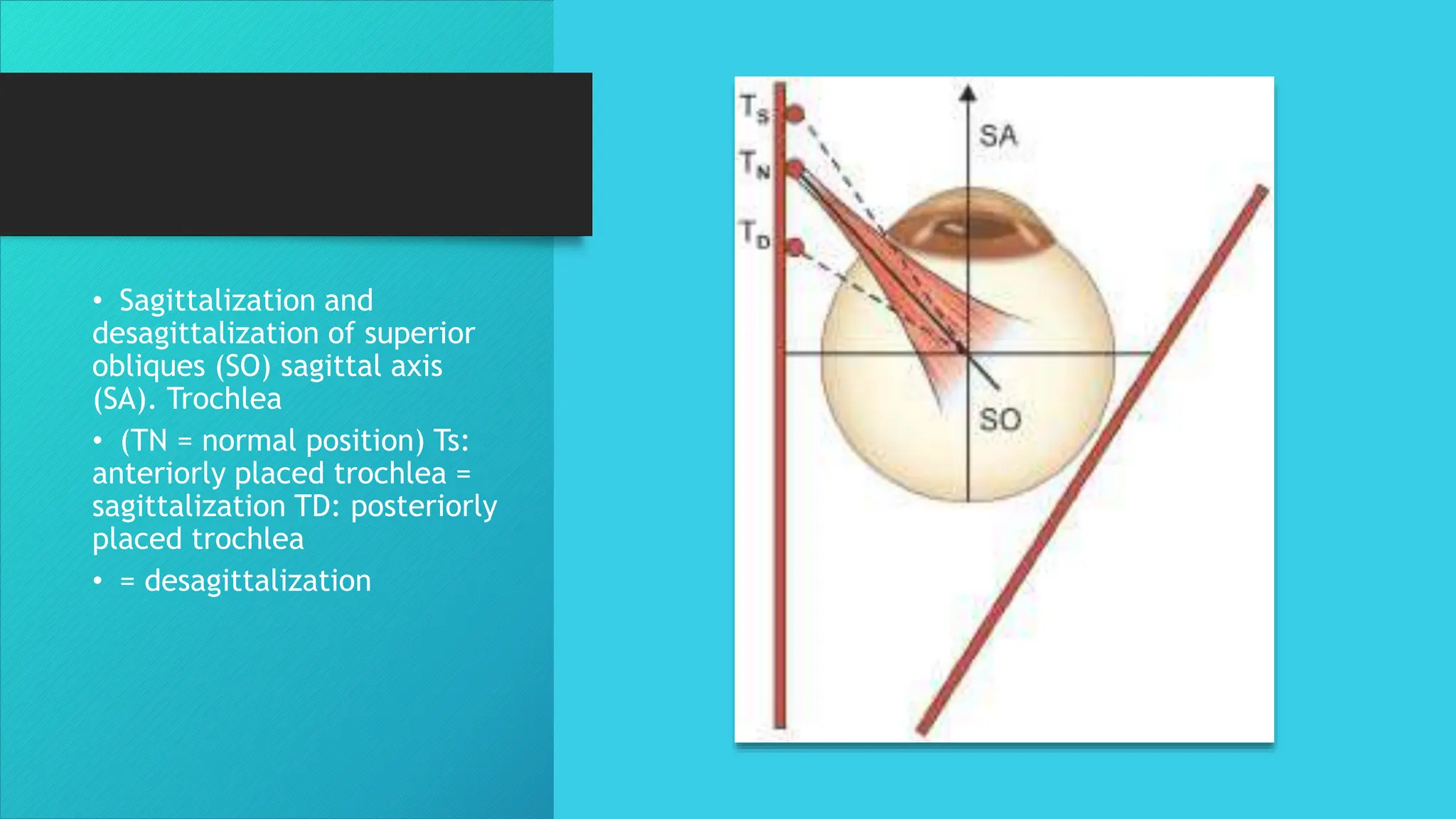
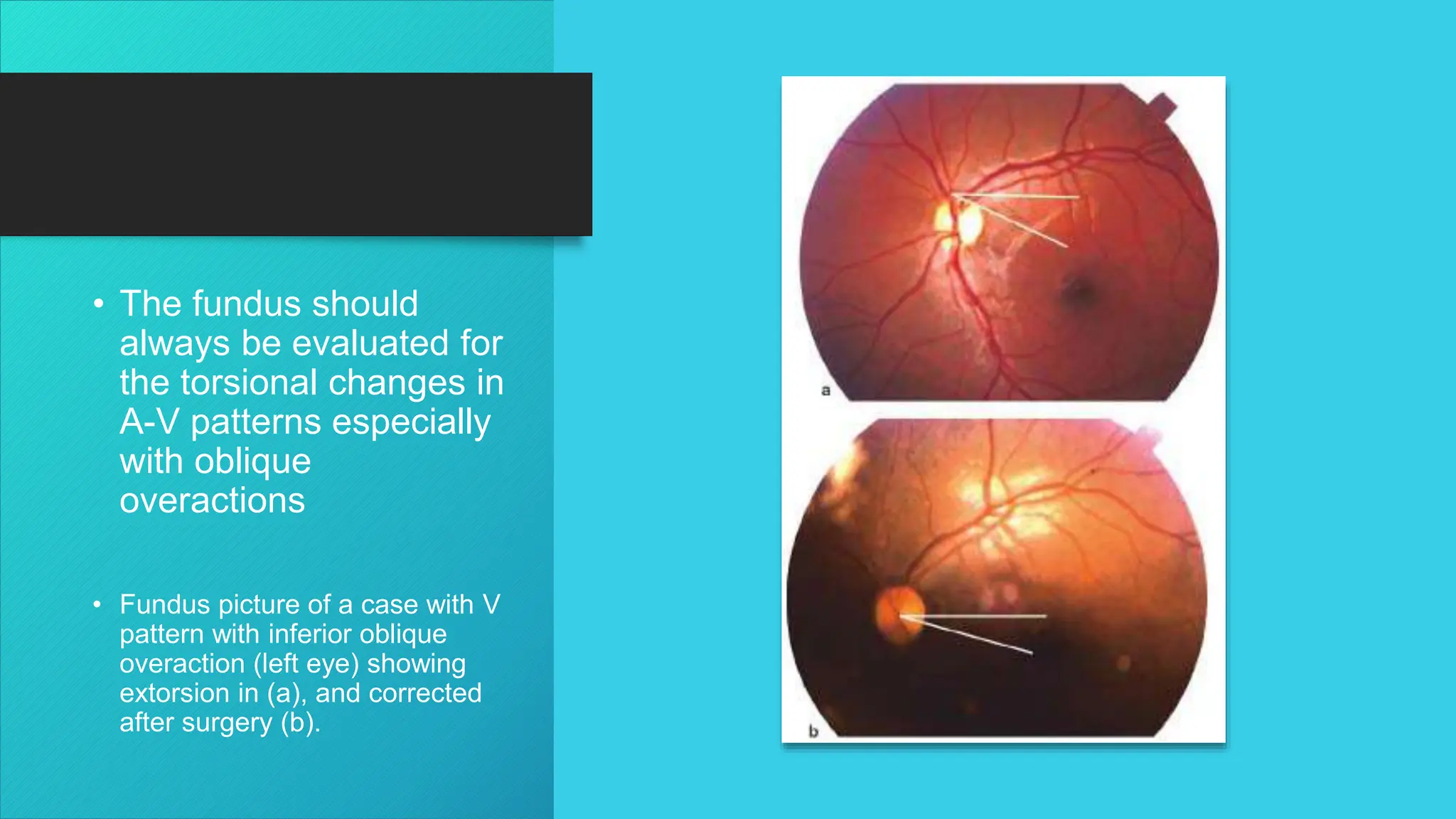
The document discusses the classifications of a and v patterns in eye deviation, emphasizing their significance in horizontal and vertical gaze. It details various types of deviations such as a-exotropia, v-esotropia, and the involvement of ocular muscles in these patterns. Additionally, it covers the diagnosis methods, prevalence among populations, and treatment options including surgical interventions for different types of patterns.