Introduction
Classificationof mandibular defects
Factors affecting treatment of mandibulectomy
patients
Relating surgical and prosthetic considerations in
mandibulectomy patients
Management of mandibulectomy patients
- Use of processed bases
- Method of recording denture space
- Removable partial denture considerations in
mandibulectomy patients
- Treatment of mandibular deviation
3.
Different typesof prosthesis used for mandibulectomy
patients
- Guide flange prosthesis
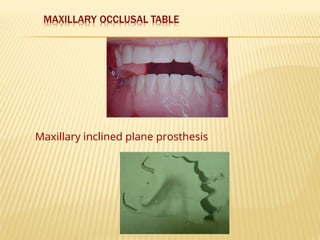
- Maxillary occlusal table
- Maxillary inclined plane
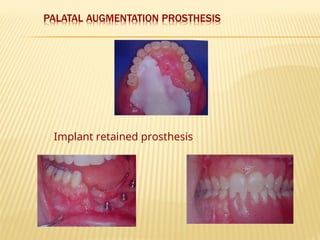
- Palatal augmentation prosthesis
- Implant retained prosthesis
Gunnings splint and stent prosthesis
Summary and Conclusion
References
5.
Classification of mandibulardefects
Based on etiology
Acc to Laney(1979)
1.Acquired: - Marginal
- Segmental - a) Lateral to midline
- Body only
- Ramus- Body with disarticulation
b) Anterior body
- Subtotal
- Total
6.
2. Congenital
- Incompleteformation
- Incomplete ossification
eg) hypoplasias, mandibulofacial dysostosis,etc
3. Developmental
as a result of postnatal insults
eg) trauma during birth, surgery,etc
7.
Continuity defect
(marginalresection)
- Inferior border and its
continuity preserved
- No deviation
- Less facial disfigurement
- Occlusion rarely changed
- Can be :- anterior defect
posterior defect
Discontinuity defect
(segmental resection)
- Complete segment of mandible from
alveolar crest to inferior border
removed
- Mandible deviates to resected
side
- Marked facial disfigurement
- Occlusion altered
- Can be :- lateral discontinuity
defect
midline discontinuity
defect
8.
Acc to Cantorand Curtis (1971)
Class 1 : Radical alveolectomy with preservation of
mandibular continuity
9.
Tissues resected :- Portion of alveolar process and body of mandible
- Lingual and buccal sulcus mucosa
- Portion of base of tongue and mylohyoid
muscle
- Lingual and inferior alveolar nerves
- Sublingual and Submaxillary salivary glands
- Sometimes anterior part of digastric muscle
FEATURES
1. Least debilitating.
2. Sometimes resection of part of mylohyoid muscle and resultant scarring
can raise the floor of the mouth causing reduction in tongue mobility.
3. Ability to shape and control the tongue may be lost due to loss of some
intrinsic muscles.
4. Resection of lingual and inf alveolar nerve results in loss of sensation to
mucosa of cheek,alveolar process,lower lip and loss of taste on anterior
2/3rd
of the tongue.
10.
Class 2 :Lateral resection of mandible distal to cuspid
11.
Tissues resected: -condyle, ramus and body of mandible distal to cuspid
- mylohyoid, hypoglossal,anterior belly of digastric, internal
pterygoid,masseter,external pterygoid, pharangoglossal
and palatoglossal muscles, most of intrinsic muscles of
tongue.
- hypoglossal , lingual and inferior alv nerves
- adjacent buccal and lingual mucosa
FEATURES
1 Speech, swallowing, saliva control, manipulation of food impaired.
2. Facial disfigurement apparent
3. Disarticulation and loss of muscles of mastication will hamper mandibular
movements
4. Taste ,sensory and motor losses more extensive as compared to class 1
12.
Class 3 -Lateral resection of the mandible to the
midline
13.
Tissues resected: all those described in class 2 in addition to the
anterior portion of the mandible, geniohyoid,
genioglossus, remaining portion of mylohyoid
muscle with lingual and buccal mucosa.
FEATURES
1. Restricted tongue mobility due to loss of tip of tongue and
genioglossus muscle
2. Speech, swallowing,saliva control and manipulation of food severely
restricted.
3. Facial disfigurement is worse due to loss of anterior part of mandible
4. Disarticulation and reduction in amount of basal bone reduce prosthodontic
prognosis.
5. Scarring of orbicularis oris can interefere with expression of emotion
Lateral boneand split thickness skin or pedicle graft can be
performed on patients who have had:
- radical alveolectomies
- resection of mandible distal to cuspid with
or without disarticulation.
3 types of bone grafts are possible
1. Mandibular augmentation procedures.
2. Bone graft that connect a residual condyle with the larger
mandibular fragment.
3. Lateral bone grafts that extend from the mandibular
fragment into the defect area to establish a pseudo TMJ.
Tissues resectedat time of orignal operation:
- anterior portion of the mandible
- large bilateral portions of mylohyoid, geniohyoid
genioglossus and anterior digastric muscles
- bilateral lingual and inferior alv nerves
- bilateral submaxillary and sublingual salivary glands
- mucosa of lower lip
- anterior floor of mouth
- ventral surface of tongue
The mucosa retained in the labial and buccal regions is sutured to the
residual stump of the tongue and a krischner wire is often positioned to
maintain the mandibular fragments .
Bone graft and split thickness skin graft or pedicle graft procedures can be
is used to restore anterior facial contour and bilateral mandibular function.
18.
Class 6: Resectionof anterior portion of the mandible
without reconstructive surgery to unite lateral
fragments
19.
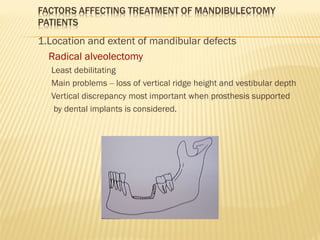
1.Location and extentof mandibular defects
Radical alveolectomy
Least debilitating
Main problems – loss of vertical ridge height and vestibular depth
Vertical discrepancy most important when prosthesis supported
by dental implants is considered.
20.
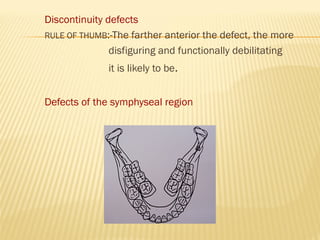
Discontinuity defects
RULE OFTHUMB:-The farther anterior the defect, the more
disfiguring and functionally debilitating
it is likely to be.
Defects of the symphyseal region
21.
Most debilitating anddifficult to treat.
Greatest facial disfigurement.
Surgical reconstruction necessary or at least segmental
stabilization before prosthodontic treatment can be
initiated.
Mandibulectomy defects in the molar region more well
suited for surgical reconstruction compared to anterior
defects.
If muscle attachments are intact – Good prognosis
Near normal appearance and function is achievable.
22.
Pts after mandibulectomypresent with few or no
remaining natural teeth.
2 reasons:
1. Pts with greatest risk of sq cell carcinoma are heavy
users of tobacco and alcohol.
2. Teeth are usually extracted prior to radiotherapy to prevent
complications such as osteoradionecrosis.
Greater the number of teeth ,better the prognosis.
Maximum number of abutment teeth should be incorporated in
the design of the prosthesis to maximise stability and dissipate
functional forces
A maxillary completedenture will function well for a
mandibulectomy patient against a reconstructed mandibular
dentition
Exceptions:
Collapse of residual proximal mandibular stump against
the posterior maxillary alveolus prohibiting adequate
denture flange extension.
When a guide flange prosthesis is planned for treatment
of mandibular deviation
25.
Deviation towards thedefect and rotation of mandibular
occlusal plane inferiorly
Deviation: Primarily due to loss of tissue involved in
surgical
resection.
26.
Rotation:Due to
- Pullof the suprahyoid muscles on the residual fragment
causing inferior displacement and rotation around the
fulcrum of the remaining condyle.
- Gravity. Loss of anchorage of elevator muscles.
Sequelae
Facial disfigurement
Loss of occlusal contact
Loss of ability to bring lips together
Drooling of saliva and difficulty to initiate swallowing
process
27.
Prosthodontic prognosisin such patients can be
improved by early post resection physical therapy to
reposition the mandibular fragment to a more normal
position and to minimize scar formation that will make
deviation more severe.
Should be carried out as early as possible.After 6-8
weeks post operatively it will not be as beneficial.
Can be in the form of
1.Physical therapy carried out by the patient himself
2.Mandibular resection guidance prosthesis
28.
Trismus –due tosurgical trauma
Physical therapy should be started immediately.
Scar tissue formation will further reduce mouth
opening.
Simple test to check mouth opening:Insert a stock
mandibular impression tray in the mouth.If this cannot
be accomplished rehabilitation will be less than
satisfactory.
Surgical intervention
29.
- Frequently thesurgical wound is closed by suturing
the remaining tissues of the floor of the mouth or
tongue to the remaining buccal tissues.
30.
This compromises: -Speech
- Swallowing
- Mastication
- Control of food bolus
- Ability to control removable
prosthesis
- Lingual vestibuloplasty and skin or mucosal grafting can
be used to improve tongue mobility
- Evaluation of tongue mobility
- In patients whom anterior resection has been done,
ability to lick the lips when the artificial prosthesis is
placed in the mouth may be difficult (due to loss of
genioglossus muscle)
31.
In such casesconsideration is given to lowering the anterior
occlusal plane or arranging the teeth slightly lingually.
Speech therapy
Loss of innervation will compromise tongue function and
prognosis of prosthodontic rehabilitation.
If lingual nerve is sacrificed during resection, the tongue on the
defect side will permanently remain without any feeling.
Loss of sensory capability:- Affects speech
Mastication
Prosthesis control
Loss of sensory innervation of the buccal mucosa(long buccal
nerve) and lower lip(mental nerve) will reduce patients ability
to control food and saliva
33.
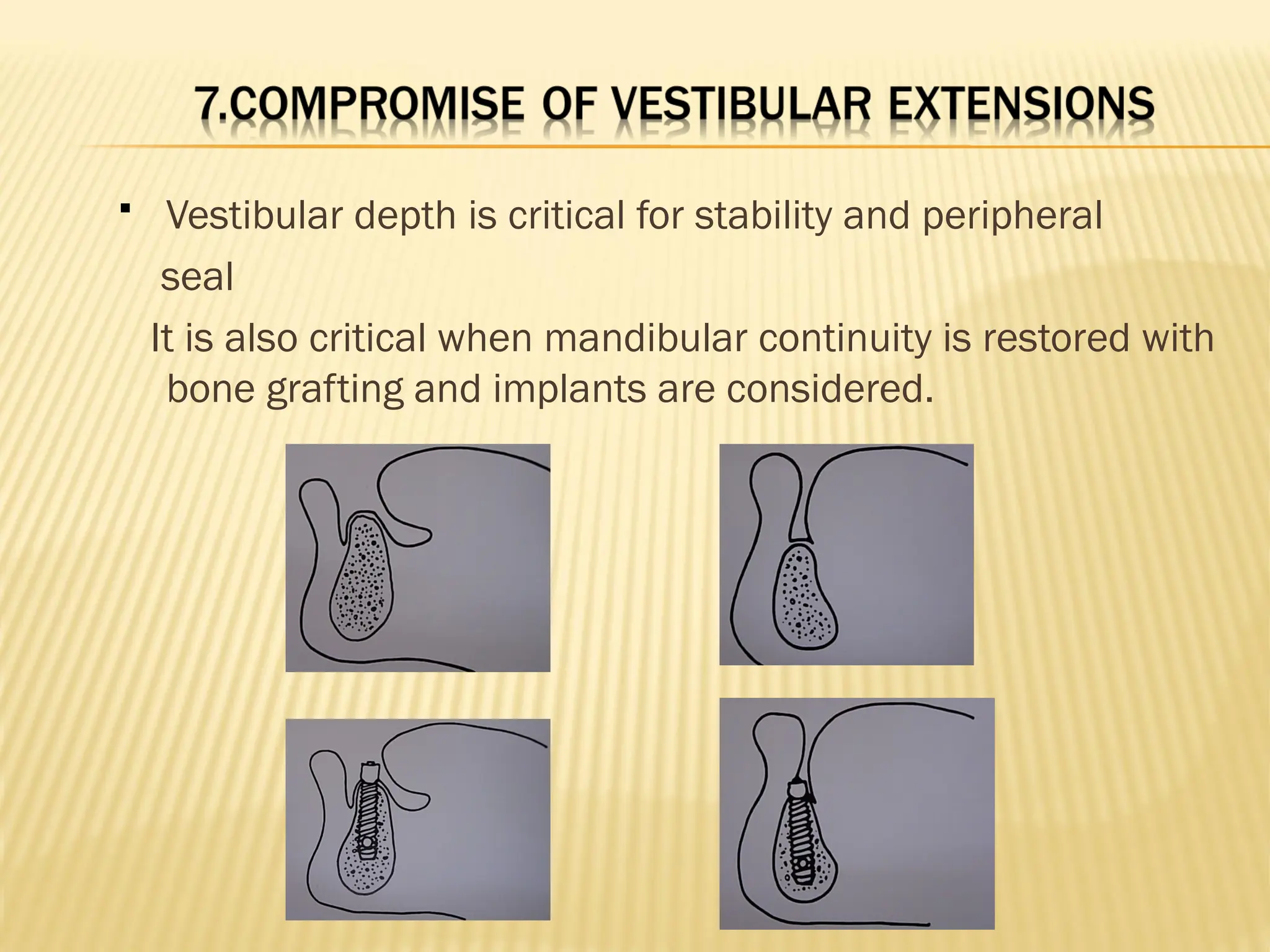
Vestibular depthis critical for stability and peripheral
seal
It is also critical when mandibular continuity is restored with
bone grafting and implants are considered.
34.
Skin graftsare used for surgical reconstruction either as lining for
the surface of resected soft tissue or as part of skin and connective
tissue grafts such as pedicle flaps, free flaps etc.
Advantages
1. Effective load bearing tissue.
2. Can withstand pressure and chafing from prosthesis.
3. Protects underlying bone and connective tissue well due to
rapid turnover of keratin producing cells.
Disadvantages
1. No sensory innervation.
2. Full thickness grafts may incorporate hair follicles.
3. Skin is not very compatible with titanium surface of implants.
35.
Careful treatmentplanning is required for
patients with radiation therapy
Irradiated tissue is fragile ,sensitive to
manipulation,dessicated,slow to heal,prone to
infection and at risk of osteoradionecrosis
36.
Reconstruction ofanterior defects
Most difficult situation for grafting and frequently results in a
graft that is deficient anteriorly.
- Results in a severe Class 2 like situation.
The prosthodontic difficulties seen in rehabilitating such a
patient
are:-
- Inability to provide proper lip support.
- Speech problems associated with mandibular dentition
placed too far lingually.
- Inability to control food bolus due to lack of motor
function of lips and lower part of the face.
37.
- Excessive displayof mandibular teeth due to patients inability
to maintain normal lip posture.
- Difficulty gaining adequate space for prosthesis placement
without encroaching on function of tongue.
- Misalignment of remaining unresected mandibular fragments
and resultant relationship between maxillary and mandibular
teeth.
Reconstruction of posterior defects
- More predictable from prosthodontic point of view as compared
to anterior defects.
- The mediolateral positon of the graft is frequently seen lateral
to the orignal position of the mandibular body. Thus the
prosthesis must be built in cross bite to maintain the denture
teeth over the supporting base of the bone graft.
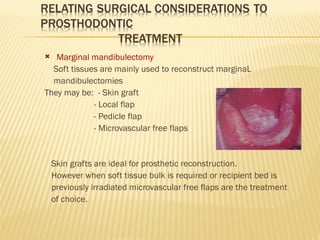
Marginal mandibulectomy
Softtissues are mainly used to reconstruct marginaL
mandibulectomies
They may be: - Skin graft
- Local flap
- Pedicle flap
- Microvascular free flaps
Skin grafts are ideal for prosthetic reconstruction.
However when soft tissue bulk is required or recipient bed is
previously irradiated microvascular free flaps are the treatment
of choice.
40.
Discontinuity defects
Previouslysoft tissue local flaps(mainly the residual
tongue sutured to the border of the defect) and pedicle
flaps (pectoralis muscle) were used.
MVFF have revolutionized the treatment of discontinuity
defects.
Microvascularized bone is mainly obtained from:
1.Fibula- most common
2.Iliac crest
Soft tissue MVFF are obtained from
1.Forearm
2.Rectus muscle
41.
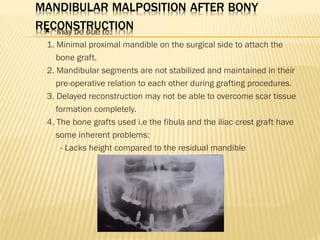
May bedue to:
1. Minimal proximal mandible on the surgical side to attach the
bone graft.
2. Mandibular segments are not stabilized and maintained in their
pre-operative relation to each other during grafting procedures.
3. Delayed reconstruction may not be able to overcome scar tissue
formation completely.
4. The bone grafts used i.e the fibula and the iliac crest graft have
some inherent problems:
- Lacks height compared to the residual mandible
42.
- Pyramidal inshape bieng narrower at the occlusal surface
- Grafted to restore inferior border of the mandible which is
necessary to restore facial form.This places it bucally in the
plane of the cheek.
- Since bone is placed bucally in the cheek implants distal to the
premolar area cause constant soft tissue and infection problems
43.
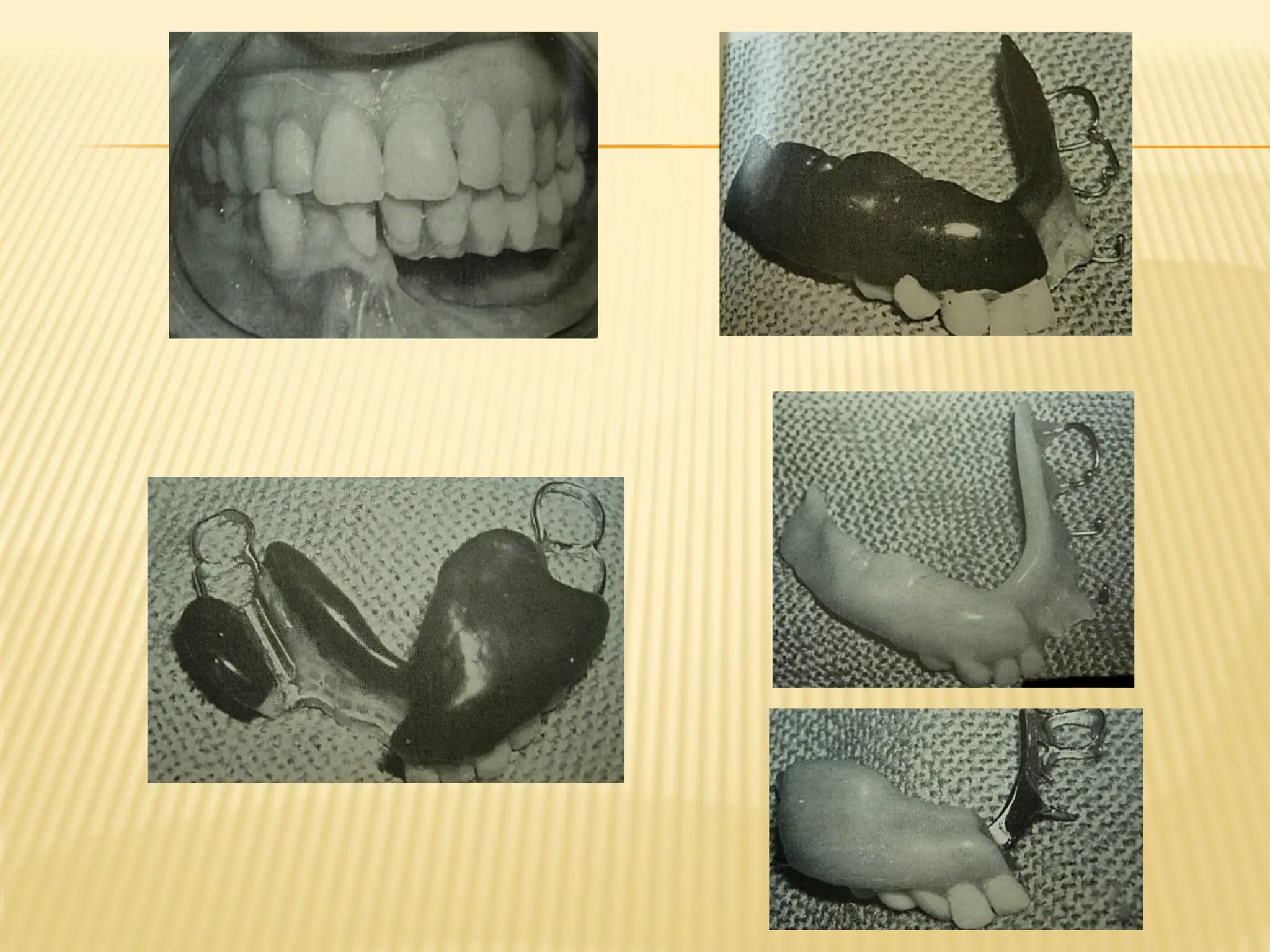
Management ofmandibulectomy patients
Processed bases
Necessary due to loss of supporting bone ,unusual intra-oral
contours,gross malposition of occlusal contacts.
Allow the determination of the relationship of the final prosthesis
periphery and the buccal or lingual tooth position.
Recording maxillo-mandibular relationship with processed bases allow
the clinician to evaluate retention and stability proir to adding wax rims
or dentition.
44.
Significant lossof alveolar bone as well as rotation and deviation
of the mandible postoperatively make it necessary for the record
bases to be as stable as possible during maxillomandibular
records.
Extension beyond the periphery of the prosthesis may be
required to support the lip.To add stability to the
prosthesis,occlusal contact may need to be significantly buccal or
lingual to normal anatomic landmarks that usually denote the
occlusal table.
Pts who have implant retained prosthesis should have
retentive elements incorporated in the processed bases.This
gives the clinician an early idea as to the support that can be
gained for the soft tissues of the face
45.
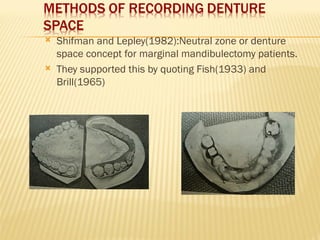
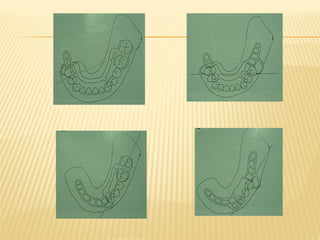
Shifman andLepley(1982):Neutral zone or denture
space concept for marginal mandibulectomy patients.
They supported this by quoting Fish(1933) and
Brill(1965)
47.
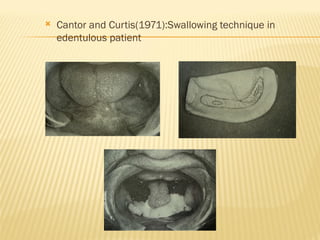
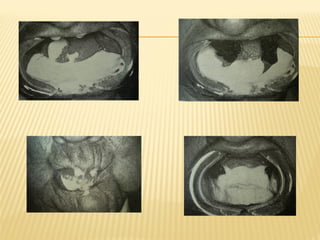
Cantor andCurtis(1971):Swallowing technique in
edentulous patient
49.
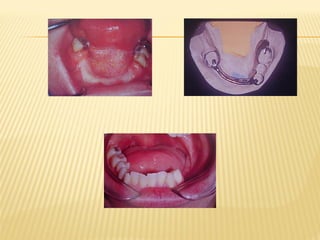
Kelly(1965):described theadvantages of using combination clasps
in mandibulectomy patients.He also described a double bar type
of stress breaker which helped maintain the partial denture in place.
52.
Review of literature
Ackerman(1955) advocated the use of intermaxillary fixation or
a guidance prosthesis immediately post operatively.The
prosthesis used a gate hinge clasp for maximum stability during
function.This design is similar to the swing lock partial denture
design.
Adisman(1962) fabricate guide plane splints that were used as
postoperative intermaxillary splints. After healing the fixed
prosthesis was replaced by a mandibular removable partial
denture guide plane.The RPD framework was made of cast
metal with a acrylic resin or heavy wire loop that extended into
the mucobuccal fold and functioned against the maxillary
posterior teeth
53.
Scanell(1965) statedthat a mandibular resection patient should
be seen by a dentist within 7-10 days.He noted that a corrective
guide flange prosthesis inserted early can avoid later difficulty in
mandibular movement.
Swoope (1969) while treating edentulous mandibular resection
patients formed a palatal ramp on the maxillary denture to
broaden the occlusal table and make it easier for the patient to
obtain stabilizing occlusal contacts.
Schaff(1976) described a removable partial denture flange
prosthesis for the patient with natural teeth. In partially
edentulous patients if teeth are strong enough, a mandibular
cast removable partial denture flange prosthesis can be used to
reduce mandibular deviation.
54.
Armany andMeyers (1977) advocated use of intermaxillary
fixation at time of surgery for 5-7 weeks.For dentulous patients if
mandibular deviation is observed after fixation, a guide flange
prosthesis can be used until the patient returns to intercuspal
position.
Desjardins(1979) stated that in dentulous patients a maxillary
palatal inclined plane palatal to the posterior teeth on the non
defect side can be used as a training device for mandibular
movement. This device is only suitable for dentulous patients.
Chalian et al(1979) indicated that a guide plane prosthesis must
be used if the resection includes the body of the mandible, ramus
and condyle.These prosthesis consist of a maxillary and
mandibular cast removable partial denture framework. A lower
inverted U shaped flange slides against a upper horizontal bar on
the non defect side.
Ackerman AJThe prosthodontic management of oral and facial
defects J Prosthet Dent,1955;5:413-432
Scannel JB Practical considerations in dental treatment of patients
with head and neck cancer J Prosthet Dent,1965;15:764-778
Kelly EK Partial denture design applicable to the maxillofacial
patient J Prosthet Dent,1965;15:168-173
Swoope CC Prosthetic management of resected edentulous
mandibles J Prosthet Dent,1969;21:197-201
Cantor R and Curtis TA Prosthetic management of edentulous
mandibulectomy patients Part 1 J Prosthet Dent,1971;25:447-455,
Part 2 J Prosthet Dent,1971;25:547-555, Part 3 J Prosthet
Dent,1971;25:671-678.
Schaff NG Oral reconstruction for edentulous patients after partial
mandibulectomies J Prosthet Dent,1976;36:292-297
61.
Armany MAand Meyers EN Intermaxillary fixation following
mandibular resection J Prosthet Dent,1977;37:437-443
Desjardins RP Occlusal considerations in partial mandibulectomy
patients J Prosthet Dent,1979;41:308-311
Shifman A and Lepley JB Prosthodontic management of
postsurgical soft tissue deformities associated with marginal
mandibulectomies J Prosthet Dent,1982;48:178-183
Clinical maxillofacial prosthetics, Thomas D Taylor;1st
edition
Maxillofacial prosthetics, Varoujan A Chalian
Maxillofacial prosthetics, postgraduate dental hand book series,Vol
4 William R Laney
Removable partial prosthodontics,Alan B Carr;11th
edition
Clinical removable partial prosthodontics,Kenneth L Stewart;2nd
edition