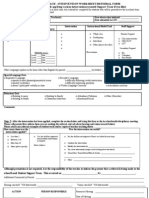
PRIORITY:
__LOW (Schedule when available) __HIGH (Schedule as soon as possible) __EMERGENCY (See now)
GUIDANCE OFFICE REFERRAL FORM
Date Received ______________
Student’s Name: ____________________________________________ Age: ______________________
Grade/Strand: _________________________________ Adviser: ________________________________
Parent/Guardian: _____________________________________ Contact No.:_______________________
Referred by:
__ Teacher __Parent __Self __Others:________________________
Reason for Referral-Problem/Concern related to: (Please check all that apply.)
( ) absences ( ) family concerns ( ) sadness
( ) academics ( ) fears ( ) self-image/confidence
( ) aggression/anger ( ) fighting ( ) social skills
( ) always tired ( ) grief ( ) stealing
( ) bullying ( ) hurts self ( ) swearing
( ) cries easily for age ( ) impulsive ( ) tardiness
( ) daydreams/fantasizes ( ) inattentive ( ) withdrawn
( ) defiant ( ) lying ( ) worries
( ) destruction of property ( ) motivation
( ) dramatic change in behavior ( ) nervous/anxious ( ) Others: __________________
( ) drop out risk ( ) over active
( ) easily distracted ( ) peer relationships
Client-Referral Problem/ History:
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Actions taken by the person referring this student, if applicable:
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Have you informed the parent/guardian about your concern? ( ) Yes ( ) No Date: __________________
Explain below the outcome of parent contact:
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
______________________________________________
Signature over Printed Name of Person Making Referral
_______________________
Date of Referral
�PRIORITY:
__LOW (Schedule when available) __HIGH (Schedule as soon as possible) __EMERGENCY (See now)
Initial date seen by the Guidance Counselor:_________________________________________________
Guidance Counselor:____________________________________________________________________
Best time to counsel the student: _________________________________________________________
Follow up session date:__________________________
Outcome:_____________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Follow up session date:__________________________
Outcome:_____________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Follow up session date:__________________________
Outcome:_____________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Follow up session date:__________________________
Outcome:_____________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Follow up session date:__________________________
Outcome:_____________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Follow up session date:__________________________
Outcome:_____________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
__________________________________
Signature of Counselor over Printed Name