0% found this document useful (0 votes)
830 views1 pageInternship Approval Form
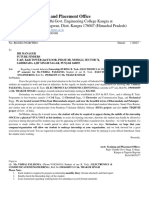
This internship approval form requires students to provide their personal details, internship organization information including address and contact of manager, expected start and end dates of minimum 6 weeks duration, and signatures of the internee, manager and internship in-charge for approval before starting the internship.
Uploaded by
mamabangoCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
830 views1 pageInternship Approval Form
This internship approval form requires students to provide their personal details, internship organization information including address and contact of manager, expected start and end dates of minimum 6 weeks duration, and signatures of the internee, manager and internship in-charge for approval before starting the internship.
Uploaded by
mamabangoCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
/ 1