0% found this document useful (0 votes)
4K views1 pageLeave Request Form PDF
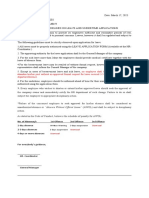
This leave request form allows an employee to request annual leave, sick leave, or other leave from their job. The employee must fill in their name, title, ID code, the dates of the requested leave, and the number of days for each type of leave. They also provide the name of who will cover their duties during their absence and emergency contact information. The form then gets approved by the employee's supervisor and hospital director before being processed by human resources to track the employee's remaining leave balances.
Uploaded by
FarhadullahCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOC, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
4K views1 pageLeave Request Form PDF
This leave request form allows an employee to request annual leave, sick leave, or other leave from their job. The employee must fill in their name, title, ID code, the dates of the requested leave, and the number of days for each type of leave. They also provide the name of who will cover their duties during their absence and emergency contact information. The form then gets approved by the employee's supervisor and hospital director before being processed by human resources to track the employee's remaining leave balances.
Uploaded by
FarhadullahCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOC, PDF, TXT or read online on Scribd
/ 1