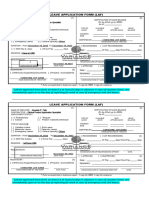
LEAVE APPLICATION FORM
General Information
Date Employee I.D. ________________________________
Applicant’s Name Designation _________________________________
Department _ Location ____________________________________
Type of Leave No. of Days Requested Reason of Leave Contact During Leave
Requested
____________________ _____________________
Casual From_______________
Sick ____________________ _____________________
Annual To_________________ ____________________ _____________________
Half Day
Hours/Days__________ ____________________ _____________________
Short Leave
CPL
Applicant’s Signature __________________
Official Use Only (To Calculate Leave Balance)
Leave Record Casual Sick Annual
Previous Balance
On This Form
Current Balance
Human Resource Remarks (If Applicable)
Remarks __________________________________________________________________________
HR Representative Name ____ HR Representative Designation ________________
Signature ________ ____ Date ________________________________________
Approving Authority (HOD / MM / MP / CEO)
Full Name Designation ______________________________________
Signature Date ______________________________________
-----------------------------------------------------------------------------
Note: Please fill the application before proceeding on leave & if it’s an emergency then call the office before
11:00 a.m. on the date of leave and fill the application form on your return day. Otherwise, you will be
consider absent. Four short leaves (short leave means maximum 2 hours leave) will be consider as one full
leave.
� Leave Approved Leave Not Approved Advice
-----------------------------------------------------------------------------
Note: Please fill the application before proceeding on leave & if it’s an emergency then call the office before
11:00 a.m. on the date of leave and fill the application form on your return day. Otherwise, you will be
consider absent. Four short leaves (short leave means maximum 2 hours leave) will be consider as one full
leave.